Welcome to Rigicon Talks, where we bring expert insights on urological prosthetics and men’s health. In this session, three leading specialists—Professor Koenraad van Renterghem (Belgium), Mr. Rowland Rees (UK), and Dr. Tobias Pottek (Germany)—answer the 10 most frequently asked questions about artificial urinary sphincters (AUS).
If you’re considering AUS as a treatment for urinary incontinence, this discussion will help you understand the procedure, benefits, and what to expect.
Frequently Asked Questions About Artificial Urinary Sphincters
1. Who is a candidate for an artificial urinary sphincter?
AUS is used to treat stress urinary incontinence (SUI) that does not respond to pelvic floor therapy or other conservative treatments.
- Stress incontinence – happens when urine leaks due to pressure on the bladder, such as coughing, sneezing, or lifting.
- After prostate surgery – common following radical prostatectomy for prostate cancer or surgery for benign prostatic hyperplasia (BPH).
- Moderate to severe incontinence – candidates typically want a permanent, reliable solution.
2. How does an artificial urinary sphincter work?
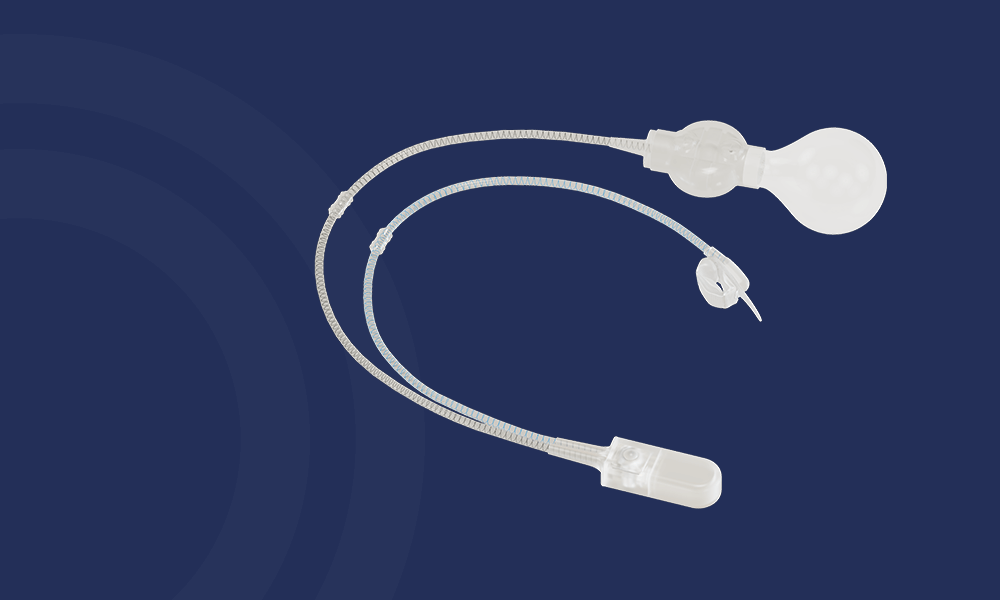
The AUS mimics the body’s natural urethral sphincter using a three-part mechanical system:
- Cuff – wraps around the urethra and keeps it closed to prevent leakage.
- Pump – placed in the scrotum; the patient presses it to release urine.
- Pressure-regulating balloon – stores and regulates fluid movement to maintain proper function.
Once the patient presses the pump, the fluid shifts, allowing the bladder to empty. After urination, the cuff automatically refills, restoring continence.
3. Can patients choose the type of AUS they receive?
Yes, but choices depend on the doctor’s expertise and product availability in your country.
There are three major brands:
- Boston Scientific® (AMS 800) – widely used, 50 years of clinical experience.
- Zephyr® (Europe-based) – newer designs with alternative pressure settings.
- Rigicon® (USA) – features adjustable pressure technology (ContiReflex®) for improved long-term function.
The right AUS is chosen based on your anatomy, medical history, and level of incontinence.
4. Will the AUS be noticeable to others?
No, the device is entirely internal.
- The cuff is placed inside the body, around the urethra.
- The balloon is positioned in the lower abdomen, where it’s not visible.
- The pump is inside the scrotum but discreet and not visible under clothing.
While the pump can be felt when touched, it does not interfere with daily activities.
5. What is the recovery time after AUS surgery?
Typical Recovery Timeline:
- 📅 Hospital Stay: Usually 1 night.
- 📅 First 1-2 weeks: Rest with minimal physical activity.
- 📅 Week 2-4: Light activities such as walking can resume.
- 📅 Week 6: The AUS is activated, and normal urination control begins.
- 📅 After 8 weeks: Patients can typically resume normal activities, including exercise.
A catheter may be used for a short period after surgery, but incontinence persists until the device is activated at the 6-week mark.
6. How should patients prepare for AUS surgery?
- Stop Smoking – Smoking increases infection risk 10 times.
- Control Diabetes – A1C levels should be below 7 to promote healing.
- Manage Blood Pressure – High blood pressure affects circulation and healing.
- Optimize Weight – A healthy weight improves post-surgery outcomes.
- Avoid Blood Thinners (if advised by your doctor).
Good pre-surgery preparation leads to better healing and long-term success.
7. How does AUS affect daily activities?
Patients can resume normal activities, including:
- ✔ Walking, running, and hiking
- ✔ Traveling and driving
- ✔ Sexual activity
- ✔ Playing sports
⚠️ Caution is needed for cycling and horseback riding, as pressure on the perineum can damage the cuff. Special cut-out seats may be recommended.
8. Are there any restrictions for MRI scans?
- AUS devices are MRI-safe.
- Most devices are tested for 1.5T and 3.0T MRI scanners.
- Always inform your radiologist that you have an AUS before an MRI.
AUS does not interfere with MRI scans or other imaging tests.
9. How long does an artificial urinary sphincter last?
Device Longevity:
- ⏳ 5-year survival rate: ~70% of devices still function.
- ⏳ 10-year survival rate: ~50% may require revision surgery.
- ⏳ 15-year survival rate: ~15% still fully functional.
🔄 Revisions may be needed due to:
- Mechanical failure (cuff, pump, or balloon).
- Urethral atrophy from long-term pressure.
- Infection (though rare with proper precautions).
Most AUS devices last 10-15 years before needing replacement.
10. What should I discuss with my doctor before getting an AUS?
Before deciding on an AUS, discuss:
- ✔ Severity of your incontinence (mild cases may benefit from male slings instead).
- ✔ Potential revision surgery – AUS may require future adjustments.
- ✔ Insurance coverage – Costs vary by region and insurer.
- ✔ Your lifestyle needs – Physical activity levels may influence device choice.
Setting realistic expectations leads to higher patient satisfaction.
Final Thoughts
AUS is a proven, effective solution for men with stress urinary incontinence. Key takeaways from this expert discussion:
For more information, watch the full Rigicon Talks – Session 2 video:
Stay tuned for more expert discussions in the Rigicon Talks series!
All trademarks, registered marks (® and ™), and product names mentioned in this article are the property of their respective owners. The use of such marks does not imply any affiliation with or endorsement by them. This content is for informational purposes only and should not replace professional medical advice. Always consult with a qualified healthcare provider before making any decisions regarding your health.