All Products
All Products

Welcome to Rigicon Academy Blog, where we dive into the latest advancements in prosthetic urology and surgical training.
In this article, we present a comprehensive transcript from a great webinar organized by the Lyx Institution, supported by the ESSM and sponsored by Rigicon®. Dr. Juan I. Martínez-Salamanca and Dr. Francois Eid moderated the meeting, with great presentations by Prof. David Ralph, Dr. Ignacio Moncada, Prof. Carlo Bettocchi, Prof. Andrew J. Stephenson, Dr. Josep Torremadé, and Dr. Agustín Fraile. Broadcasted on December 16, 2021.
Opening Remarks
Hello, good evening in Europe, or good afternoon in the US, or good morning in some parts of the world, or even good night in Asia and the Middle East. It’s my pleasure to present to you today this new course seminar on New Frontiers in Surgical Innovation: Prosthetic Urology—What’s Up?
I think we have some new players in the field in recent months, and this is the main reason why I would like to share this seminar with you today. I’d like to especially thank the ESSM, the European Society of Sexual Medicine, for their support in making this initiative possible, and also Rigicon® as the main sponsor. A big thanks to Marcus, Rafael, and everyone at their team for this extraordinary work in organizing this live webinar.
I’d also like to thank our partners Educamet, especially Belen Fernandez, who helped all of us—the speakers and organizers—with logistics and arrangements for this course. I’d like to introduce my co-moderator. It’s my pleasure to present Dr. Francois Eid. He’s a urologist, very well known, a world-class expert in prosthetic surgery, working in the field for many years. He’s joining us from New York, from Advanced Urological Care. Thank you, Dr. Francois Eid.
Thank you, Dr. Juan I. Martínez-Salamanca, it’s a pleasure to be here. Thank you for the invitation. We have a great group of doctors that you’ve put together, which is really exciting. I also want to thank Rigicon® for allowing me to participate in this international meeting, and I look forward to listening to all the presenters.
New Developments and Tools in Penile Implants
Well, thank you very much for inviting me to be part of this webinar. I’m going to talk about the new developments and tools that we have in penile implants. I think gone are the days—or soon gone are the days—of using just Hegars or Brooks dilators. We have new dilators coming along now. Here are just a few examples. On the left, you can see the Morville Euromix dilators, nicely graduated with olive tips. One of the best dilators we have now are the Rigicon® HL dilators, which, as you can see, look a bit like Brooks. You can have it as a set of three, or, as I do, just have one with a 10-olive tip on one end and a 12-olive tip on the other.
I tend only to dilate once or twice, but the nice thing is it’s graduated, so you don’t need to put your Furlow in to measure and then take it out again. You can pass this dilator up—use the 10, then move to the 12—and do your measurements as you go. It’s also available as a disposable set, which we’re probably going to move toward in the future because disposable instruments may reduce infection risk.
Cabinotomes remain crucial: we have Cabot, Homes, and Rossello versions, among others, and we use them carefully in tougher cases. My standard tray only has one standard dilator for virgin cases, and if I have difficult fibrosis, I have the Euromix cabinotomes. I have a Furlow and some backward-cutting scissors, which can be quite useful in cases of fibrotic tissue, to open the corporotomies. Having disposable tools such as retractors and hooks can also be handy. Rigicon® does a very nice set—equal rings, snowman shape, rectangular shape—depending on your operation. The good thing now is you open the box and you get a retractor, a Furlow, your dilators, and so on, hopefully all disposable.
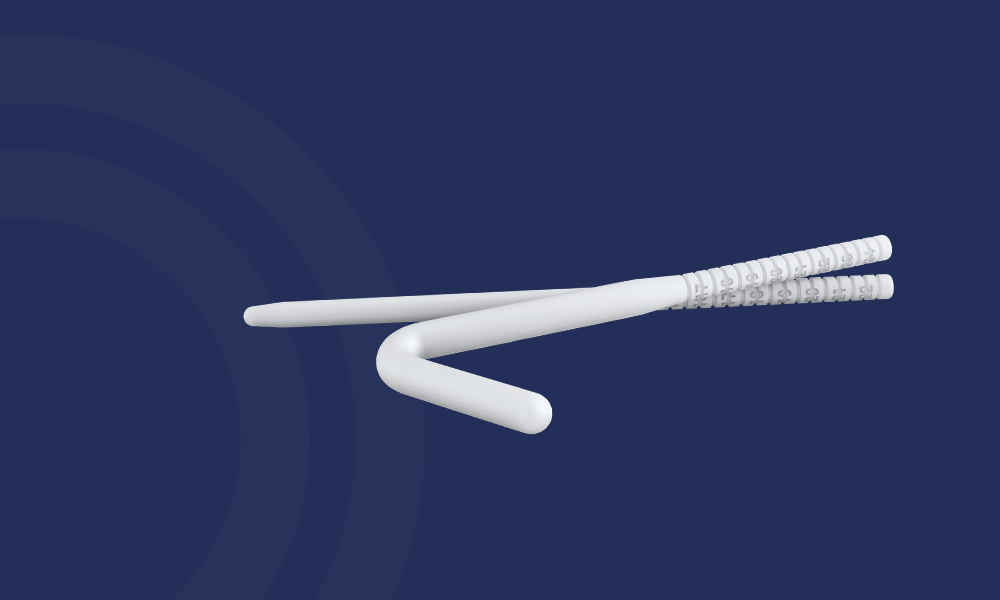
What’s new on the market? Malleables. The workhorse is the Genesis from Coloplast®. A year or so ago, we got the Tactra™ from Boston Scientific®, which some like because it’s stiffer. In between these might be the Rigicon® Rigi10™, with very nice soft tips. You can dip it in antibiotic solution. It comes in different sizes—9, 10, 11, 12, 13—so you have flexibility without ordering separate kits. Only two malleables on the market—Rigicon® and Tactra™—are coated to help reduce infection risk. Rigicon® also has a lifetime warranty, which patients like.
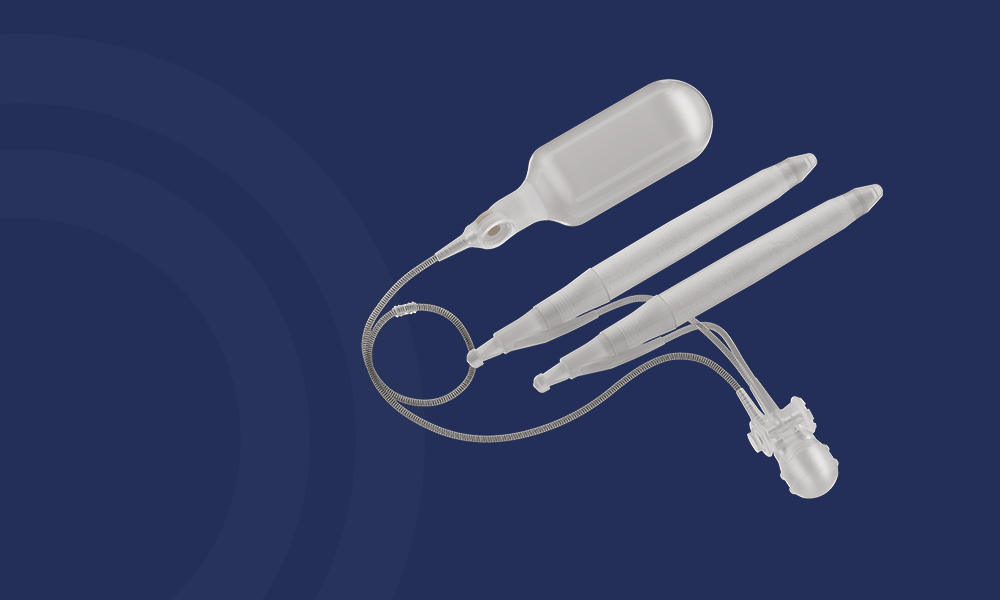
On inflatable implants, we traditionally had the Coloplast® Titan™ or the Boston Scientific® AMS 700™. Rigicon® now has a series, the Infla10®, which comes in three varieties: standard, AX (length and girth expansion), and Narrow Base. The Rigicon® pump’s deflate button stands out a bit more, so for patients who might have dexterity issues, that’s good. The reservoir has a sunken lockout valve to help reduce auto-inflation. Overall, it’s nice: it’s pretty soft in flaccid state, yet it develops good rigidity, likely thanks to a four-layer design. Ultimately, we want to see how they fare long-term. We also have the Zephyr® line for transgender patients, which includes a malleable or single-cylinder inflatable with a base plate attached to the pubic symphysis. The future might bring the first electronic IPP, and then others will follow.
We also see new ectopic reservoir placement techniques to prevent herniation. For example, a McClintock™ clamp helps dilate without enlarging the superficial ring. There’s also a modeling device for Peyronie’s disease. Some use at-home modeling after a mild residual curvature—patients basically keep modeling postoperatively to hopefully reduce the need for complicated maneuvers. We suspect the era of extensive sliding techniques is diminishing because of complications. The multi-slit technique might still be considered, but let’s see.
Thank you very much.
Discussion on New Implants
“Thank you, excellent talk. That was very good. Thank you for this great overview of new devices. From your personal experience, for example, what’s your feeling with the new Rigicon® instruments?”
I think these are nice minor changes in devices we’ve had. For instance, you mention the disposable Furlow. We found, in a study, that cleaning Furlows is tricky, and about 2.4% tested positive for staph contamination. So, imagine reusing that in a surgery. The new disposable Furlows might help. Same with disposable dilators. It might mean less contamination overall.
Managing Infection, Satisfaction, and Challenging Cases
Hello, everybody, my name is Ignacio Moncada. I’m a urologist, chief of urology and andrology at a hospital in Madrid, Spain. Thank you for the invitation to Juan Ignacio Martinez and all the Lyx Institution for having me. My talk today is on How to Improve Outcomes: Infection, Patient Satisfaction, and Challenging Patients. I’ll make a brief review on these topics.
Patient Satisfaction and Expectations
Patient satisfaction after surgery often depends on the patient’s experience versus their expectations. If the expectation is too high, even a good outcome can feel disappointing. Satisfaction with penile implants is generally 90% or more. If a patient is satisfied, so is their partner, and usually so is the doctor. But a bad outcome—or even a good outcome with unrealistic expectations—can be a major problem. That’s why Steven K. Wilson frequently advises: “Under-promise but over-deliver.”
Be careful with challenging (or “cursed”) patients: compulsive, never happy, penocentric, or those with unrealistic demands. They might push for revisions when it’s not truly indicated or do “surgeon shopping.” They can also have psychiatric disorders that complicate matters.
Causes of Dissatisfaction
Key issues include:
-
Perceived Penile Shortening: especially in Peyronie’s disease or post-radical prostatectomy or in men with BMI over 30.
-
Cold Glans: the implant doesn’t address glans engorgement.
-
Infection: though overall rare, it can be severe if it occurs.
-
Mechanical Failures: though better now, it’s still a possibility.
-
Partner Issues: dissatisfaction if the partner perceives changes they dislike.
Penile Length
Many men feel their penis is shorter, even if objective measurements show minimal change. Measuring properly is important—patients should measure after inflation and sexual arousal, as glans engorgement can add up to 20–30% length. Some men might be better served doing a vacuum or traction routine a few weeks preoperatively to preserve or gain length.
Infection Risks
Penile implant infections are generally opportunistic staph species, with toxic bacteria (like E. coli) less common. Infection in a virgin implant without risk factors is under 1%. If infection does occur, it can present as a low-grade infection (mild signs, maybe a sinus tract) or a toxic infection (fever, deep abscess). Low-grade infections may be salvageable via the Mulcahy technique—removing the device, washing with antibiotic solutions, then placing a new implant. High-grade “toxic” infections often require complete removal and waiting months before re-implantation.
Mechanical Reliability
Modern implants are more mechanically reliable than in decades past. Ten-year survival rates can approach 75–95%. Failures can involve fluid leakage, pump malfunction, or auto-inflation issues. MRI can help diagnose mechanical or structural issues, such as a cylinder’s buckling or aneurysm.
Managing Fibrosis or Difficult Cases
When re-implanting after infection or in fibrotic Peyronie’s disease, some surgeons use smaller cylinders (CX or narrower base) or specialized cabinotomes (disposable or Morville). Sometimes, removing scar tissue and using antibiotic-impregnated implants is recommended.
Conclusion
Since the introduction of penile prostheses many years ago, multiple modifications and new brands have increased mechanical reliability, prevented infection, and improved patient satisfaction. Implant selection and surgical approach should be based on patient anatomy, expectations, and ability to manipulate the device. Recognizing complications and challenging patients is critical for a satisfactory outcome. Techniques such as vacuum or traction therapy beforehand, as well as thorough discussions of realistic expectations, can help maximize satisfaction and restore a confident, healthy sex life.
Counseling and Expectations
Hello, this is Carlo Bettocchi. Thank you to my friends at Lyx and Rigicon® for inviting me. I’m talking about How I Talk to Patients About Penile Implants: Managing Expectations.
In the guidelines, penile implants are third-line therapy, offered when first- and second-line medical treatments fail or become unsatisfactory. Yet 50–80% of patients may abandon medical therapy within the first year, often citing side effects, cost, or the desire for a permanent fix. Penile implants uniquely offer a complete resolution of ED, but they’re irreversible, so preoperative counseling is vital.
Challenges often include fear of decreased sensation or an unnatural look, changes in orgasm, or concerns about safety. Realistically, orgasm and ejaculation are generally unchanged, but the glans might not be as engorged. Our job is to mold expectations and correct misconceptions.
Cold Glans is a common concern; we explain that the implant occupies the corpora cavernosa, but not the glans. We can manage it with intraurethral alprostadil, or patients can use PDE5 inhibitors if they have partial function. There’s also mention of selective venous ligation, but that’s more complex.
Penile Shortening: Some 30% of men report feeling shorter. We often measure the penis before surgery to have objective data. Some devices, like the AMS LGX™, can expand in length and girth, which can help. If we measure preoperatively, we minimize confusion afterward. Also, using vacuum or traction preoperatively can gain 1–2 cm of length.
Satisfaction is generally 90% and higher, with many men reporting better self-esteem, sense of virility, and improved relationships. Partners also tend to report high satisfaction, feeling intercourse is restored to normal. I mention that 15–20 years later, many men still have the device working well and remain happy.
Take-Home Messages: Penile implants are a gold-standard solution for advanced ED. Improved technology and surgical techniques have raised success and satisfaction. But correct pre-, intra-, and postoperative management—and especially proper patient education—are crucial to successful outcomes.
Robotic Surgery as a Disruptive Innovation
Greetings, I’m Andrew Stephenson, Professor of Surgery and Head of Urologic Oncology at Rush University in Chicago. While I’m not a prosthetic specialist, I’m heavily involved in surgical innovation from oncology and robotics perspectives. Robotic surgery was once criticized as offering no real advantage over open approaches, yet it disrupted the field by appealing to patients’ desire for minimally invasive methods and eventually became the standard of care. This concept of a ‘disruptive innovation’ reveals how new technology can start off seemingly inferior but, over time, surpass established methods and dominate the market. The parallel is that in prosthetic urology, new disposable instruments and advanced designs may follow a similar path, eventually outpacing older methodologies as they improve usability, reduce costs, and lower infection risks.
Final Thoughts
Technological innovations—from robotic approaches in oncology to novel disposables and advanced penile implant designs—will continue to expand the boundaries of what’s possible in surgical care. However, success depends on adequate counseling, realistic patient and partner expectations, and skilled technical execution. Whether it’s the cold glans phenomenon, infection management, or mechanical reliability, thorough communication with patients, meticulous surgical technique, and experience remain paramount for optimal outcomes.
Thank you very much again for your attention, and we look forward to future innovations that will further refine surgical solutions in urology.
🩺 Stay tuned for more insights from the frontlines of urologic innovation.
All trademarks, registered marks (® and ™), and product names mentioned in this article are the property of their respective owners. The use of such marks does not imply any affiliation with or endorsement by them. This content is for informational purposes only and should not replace professional medical advice. Always consult with a qualified healthcare provider before making any decisions regarding your health.